Radiation Oncology/CNS/Germinoma
|
CNS Germinoma
Overview
edit- Rare primary CNS tumor, 3-5% of childhood brain tumors
- Typical age at presentation is early teens
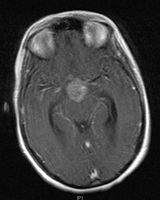
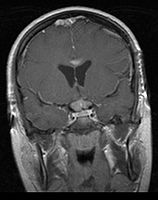
- Mainly located in midline structures, suprasellar region or pineal gland, also basal ganglia and hypothalamus
- Can be M+ in as much as 24% histologically verified cases; Disease outside of CSF is very rare
- Bifocal germinomas (synchronous suprasellar and pineal tumors) regarded as M+ in USA but M0 in Europe
- Natural spread believed to be along subependymal lining of 3rd and 4th ventricles, leading to intraventricular relapse before spinal dissemination
- Very sensitive to both radiation and chemotherapy
Location
edit- Pineal Gland Germinoma
-

-



- Suprasellar Germinoma
-
-

-



Treatment
edit- Treatment of M0 disease is somewhat controversial. Historically craniospinal RT was the gold standard, but with local control >99% and 10-year survival rates >90%, limiting side-effects is essential.
- There is now a movement toward WBRT, and further to tumor + ventricles only. Isolated spinal relapse appears comparable between CSI and whole-brain RT or whole-ventricular RT with neoadjuvant chemo
- Focal RT of primary tumor alone appears associated with significantly higher overall and isolated spinal relapse
- M+ disease continues to be treated with CSI
- Attempts at treatment with chemotherapy alone have resulted in ~50% relapses and ~10% treatment-related mortality; which is much worse than RT alone. This is currently not recommended
- Current RT approach (1/11, PMID 20452141):
- Whole ventricular volume: 3rd, 4th, lateral, prepontine cistern
- Involved field volume: pre-chemotherapy volume + clinical margin 1-1.5 cm
- Dose to primary disease is typically 40-45 Gy, and to subclinical disease 20-24 Gy
- Review PMID 15992700 -- "Radiotherapy of localised intracranial germinoma: time to sever historical ties?" (Rogers SJ, Lancet Oncol. 2005 Jul;6(7):509-19.)
- Reviewed 20 studies since 1988. 788 patients. 66% cases histologically confirmed, 12/20 series 100% confirmation. Median F/U 6.4 years
- CSI: local control 99.7%; relapses 3.8% but half of them outside CS axis; isolated spinal relapse 1%
- WBRT or Whole-ventricular RT+boost: both comparable. local control 97%; relapses 8%; isolated spinal relapse 3%
- Focal: local control 93%; relapses 23%; isolated spinal relapses 11%
- Conclusion: Whole-ventricular RT + boost should replace craniospinal RT in completely staged localized intracranial germinomas
Treatment of relapses:
Chemotherapy.
Studies
edit- Seoul; 2008 (1981-2003) PMID 18514777 -- "Upfront chemotherapy and involved-field radiotherapy results in more relapses than extended radiotherapy for intracranial germinomas: modification in radiotherapy volume might be needed." (Eom KY, Int J Radiat Oncol Biol Phys. 2008 Jul 1;71(3):667-71.)
- Retrospective. 81 patients with tissue-confirmed intracranial germinoma. 39 RT only (all CSI), 42 chemo-RT (size depended on tumor extent, ranging from tumor only to CSI). Median F/U 5.7 years
- Outcome: 5-year OS RT 100% vs. chemo-RT 93%; 5-year RFS RT 100% vs. 88% (SS). 4 relapses in chemo-RT group (3 in brain and 1 in spine)
- Toxicity: same proportion return to school (NS), hormonal therapy RT 69% vs. chemo-RT 38%
- Conclusion: Better quality of life in chemo-RT but worse relapse compared with RT alone. Primary tumor RT not sufficient, suggest at least inclusion of ventricles
- POG 9530 (1997-1999) -- response-based RT
- Phase II. 12 germinoma patients (and 14 NGGCT patients and/or elevated AFP/bHCG - not further discussed here). Age >3 years. 5 resected, 7 bx. Germinoma treated with cisplatin/etoposide and vincristine/cyclophosphamide x4 cycles. If CR, primary site RT 30.6 Gy; if PR primary site RT 50.4 Gy with 2cm margin (3D-CRT) or 0.5cm margin (SRT). If disseminated disease and CR, CSI 30.6 Gy; if PR CSI 36 Gy
- 2007 PMID 16598761 -- "Pre-radiation chemotherapy with response-based radiation therapy in children with central nervous system germ cell tumors: a report from the Children's Oncology Group." (Kretschmar C, Pediatr Blood Cancer. 2007 Mar;48(3):285-91.)
- Outcome: 11/12 progression-free at median 5.5 years, 1/12 refused RT, failed at 10 months, RT salvage, progression-free at 4.8 years
- Conclusion: Response (91%) and survival encouraging
- Toronto; 2006 (1995-2004) PMID 16530340 -- "Limited-field radiation for bifocal germinoma." (Lafay-Cousin L, Int J Radiat Oncol Biol Phys. 2006 Jun 1;65(2):486-92.)
- Retrospective. 6 patients with bifocal germinoma (pineal + suprasellar). All with diabetes insipidus at presentation. Treated with chemo followed by limited-field RT (whole ventricle 24-40 Gy +/- boost). Median F/U 4 years
- Outcome: 100% complete remission
- Conclusion: Bifocal germinoma can be considered locoregional rather than metastatic disease
- MAKEI 83/86/89, 1983-93 (German) - MAKEI = Maligue Keimzelltümoren (malignant germ cell tumors)
- Prospective, non-randomized. Goal: dose reduction. 60 pts. Germinomas. Three trials: 83(pilot) and two successive trials. Biopsy only (no resection)
- In MAKEI 83/86 (11 pts), RT to 36 Gy to craniospinal axis + 14 Gy boost to tumor (total 50 Gy, at 1.8-2 Gy/fx). In MAKEI 89 (49 pts), 30 Gy (CSI) + 15 Gy (total 34 Gy at 1.5 Gy/fx).
- PMID 10561326, 1999 — "Radiation therapy for intracranial germinoma: results of the German cooperative prospective trials MAKEI 83/86/89." Bamberg M et al. J Clin Oncol. 1999 Aug;17(8):2585-92.
- Mean f/u 59 mos. CR in all pts. 5-yr RFS 91%, OS 93%
- Conclusion: dose reduction is feasible.
- SIOP CNS GCT 96
- CSI 24 Gy
- MSKCC; 1996 PMID 8918487 -- "Chemotherapy without irradiation--a novel approach for newly diagnosed CNS germ cell tumors: results of an international cooperative trial. The First International Central Nervous System Germ Cell Tumor Study." (Balmaceda C, J Clin Oncol. 1996 Nov;14(11):2908-15.)
- Prospective. 68/71 patients (45 germinoma, 26 NGGCTs). Chemo carboplatin, etoposide, bleomycin x4 cycles. If CR, 2 more cycles. If PR, 2 more cycles intensified by cyclophosphamide.
- Outcome: CR rate germinomas 86%, NGGCT 78%. 2-year OS germinoma 84%, NGGCT 62%
- Toxicity: 7/71 patients (10%)
- Conclusion: Chemo-only regimens should be used only in setting of clinical trials
- Seoul; 1996 (Korea)(1980-1996) PMID 8850422 -- "Radiotherapy of intracranial germinomas." (Huh SJ, Radiother Oncol. 1996 Jan;38(1):19-23.)
- Retrospective. 32 patients, confirmed intracranial germinomas (14 suprasellar, 12 basal/thalamus, 4 pineal, 2 multiple). CSI in 29 patients. RT tumor bed 54 Gy, whole-brain 36 Gy, spinal axis 24 Gy
- Outcome: 5-year OS 97%, 10-year OS 97%; 1 death with persistent tumor 2 months after RT; no intracranial or spinal recurrence
- Toxicity: 1 severe intellectual deterioration, 3 vertebral growth impairment
- Conclusion: Excellent result with RT alone
Proton Therapy
edit- Harvard; 2010 (1998-2007) PMID 20452141 -- "Proton Radiotherapy for Pediatric Central Nervous System Germ Cell Tumors: Early Clinical Outcomes." (Macdonald SM, Int J Radiat Oncol Biol Phys. 2010 May 6. [Epub ahead of print])
- Retrospective. 22 patients, CNS germ cell tumors, treated with 3D PT. Patients also replanned with IMRT and IMPT. Median F/U 2.3 years
- Outcome: Local control 100%, no CNS recurrences, PFS 95%, OS 100%
- Treatment planning: Comparable CTV coverage with IMRT, 3D-CPT, and IMPT. Substantial normal tissue sparing with either PT over IMRT. IMPT may yield additional brain and temporal lobe sparing
- Conclusion: Preliminary disease control favorable; superior dose-distribution compared to IMRT